

Knee Replacement Surgery
Knee replacement surgery — also known as knee arthroplasty (ARTH-row-plas-tee) — can help relieve pain and restore function in severely diseased knee joints as a result of osteoarthritis and joint degeneration. Knee replacement surgery involves cutting away damaged bone and cartilage from your thighbone, shinbone and kneecap and replacing it with an artificial joint (prosthesis) made of metal alloys, high-grade plastics and polymers.
The most common cause of chronic knee pain and disability is arthritis. Although there are many types of arthritis, most knee pain is caused by just three types: osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis.
Osteoarthritis. This is an age-related "wear and tear" type of arthritis. It usually occurs in people 50 years of age and older, but may occur in younger people, too. The cartilage that cushions the bones of the knee softens and wears away. The bones then rub against one another, causing knee pain and stiffness.
Rheumatoid arthritis. This is a disease in which the synovial membrane that surrounds the joint becomes inflamed and thickened. This chronic inflammation can damage the cartilage and eventually cause cartilage loss, pain, and stiffness. Rheumatoid arthritis is the most common form of a group of disorders termed "inflammatory arthritis."
Post-traumatic arthritis. This can follow a serious knee injury. Fractures of the bones surrounding the knee or tears of the knee ligaments may damage the articular cartilage over time, causing knee pain and limiting knee function.
At Aptiva Health, we offer same-day and walk-in appointments for knee injuries and conditions to evaluate, diagnose, and make the appropriate referral for additional treatment based upon your specific knee injury or condition. We treat these conditions in our General Medicine, Orthopedics, Sports Medicine, Pain Management, and Physical Therapy departments.

Description of Surgery
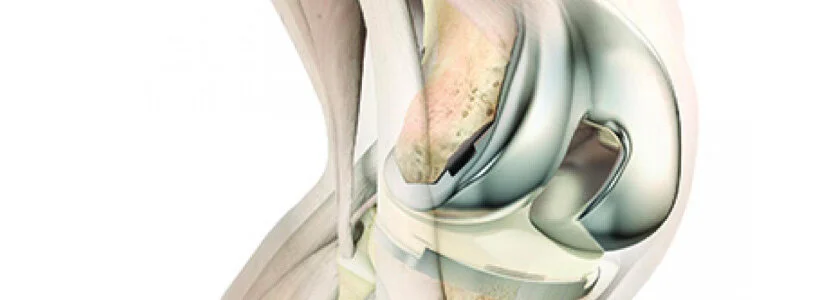
A knee replacement (also called knee arthroplasty) might be more accurately termed a knee "resurfacing" because only the surface of the bones are replaced.
There are four basic steps to a knee replacement procedure:
Prepare the bone. The damaged cartilage surfaces at the ends of the femur and tibia are removed along with a small amount of underlying bone.
Position the metal implants. The removed cartilage and bone is replaced with metal components that recreate the surface of the joint. These metal parts may be cemented or "press-fit" into the bone.
Resurface the patella. The undersurface of the patella (kneecap) is cut and resurfaced with a plastic button. Some surgeons do not resurface the patella, depending upon the case.
Insert a spacer. A medical-grade plastic spacer is inserted between the metal components to create a smooth gliding surface.
How is a total knee replacement performed?
First, the orthopedic surgeon makes an incision (cut) in the knee and moves the patella (kneecap) to the side. If are any bone spurs (small bony growths) are present, as sometimes occurs in osteoarthritis, they will be removed.
Next, the two menisci between the femur and tibia are removed, as are the anterior cruciate ligament (ACL) and, in some cases, the posterior cruciate ligament (PCL). In some types of knee replacement, the PCL is retained.
During the main phase of the operation, the surgeon cuts and remove cartilage and some bone from the upper part of the tibia and lower sections of the femur. The femoral sections removed are two knobby protuberances called the femoral condyles. The tibia and femur are then be capped with metal implants to create new surfaces for the joint. The surface of the femoral component mimics the shape of the original femoral condyles. If the kneecap has also degraded, the surface on its underside may also be cut away and replaced with a polyethylene implant.
Finally, the various layers of tissue are repaired with dissolvable sutures and the skin incision is closed with sutures or surgical staples. A bandage will be wrapped around the knee and the patient is be taken to recovery.
What are knee replacement implants made of?
The selection of knee replacement prosthesis design and materials depends on each individual patient. The main implant components are made of metal – usually titanium or chrome-cobalt alloys. The implants are fixated in place either with a cement bonding agent or by osseointegration, in which a porous metal stem extends into the tibia and the patient's natural bone grows into it. A plastic platform or spacer will be inserted between the tibial and femoral implant surfaces. The spacer is made of polyethylene.
Most femoral components are made of metal alloys (cobalt chromium) or metal-ceramic alloys (oxidized zirconium). The patellar component is plastic (polyethylene). The tibial insert component is also plastic (polyethylene). The tibial tray component can be made of the following materials:
cobalt chromium (metal alloy)
titanium (metal alloy)
polyethylene (plastic)

After Surgery
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster. Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Blood Clot Prevention
Your orthopedic surgeon may prescribe one or more measures to prevent blood clots and decrease leg swelling. These may include special support hose, inflatable leg coverings (compression boots), and blood thinners. Foot and ankle movement is also encouraged immediately following surgery to increase blood flow in your leg muscles to help prevent leg swelling and blood clots.
Physical Therapy
Most patients can begin exercising their knee hours after surgery. A physical therapist will teach you specific exercises to strengthen your leg and restore knee movement to allow walking and other normal daily activities soon after your surgery.
To restore movement in your knee and leg, your surgeon may use a knee support that slowly moves your knee while you are in bed. The device is called a continuous passive motion (CPM) exercise machine. Some surgeons believe that a CPM machine decreases leg swelling by elevating your leg and improves your blood circulation by moving the muscles of your leg, but there is no evidence that these machines improve outcomes.
Your Recovery at Home
The success of your surgery will depend largely on how well you follow your orthopedic surgeon's instructions at home during the first few weeks after surgery.
Wound Care
You will have stitches or staples running along your wound or a suture beneath your skin on the front of your knee. The stitches or staples will be removed several weeks after surgery. A suture beneath your skin will not require removal. Avoid soaking the wound in water until it has thoroughly sealed and dried. You may continue to bandage the wound to prevent irritation from clothing or support stockings.
Diet
Some loss of appetite is common for several weeks after surgery. A balanced diet, often with an iron supplement, is important to help your wound heal and to restore muscle strength.

Activity
Exercise is a critical component of home care, particularly during the first few weeks after surgery. You should be able to resume most normal activities of daily living within 3 to 6 weeks following surgery. Some pain with activity and at night is common for several weeks after surgery.
Your activity program should include:
A graduated walking program to slowly increase your mobility, initially in your home and later outside
Resuming other normal household activities, such as sitting, standing, and climbing stairs
Specific exercises several times a day to restore movement and strengthen your knee. You probably will be able to perform the exercises without help, but you may have a physical therapist help you at home or in a therapy center the first few weeks after surgery.
You will most likely be able to resume driving when your knee bends enough that you can enter and sit comfortably in your car, and when your muscle control provides adequate reaction time for braking and acceleration. Most people resume driving approximately 4 to 6 weeks after surgery.

Your New Knee Is Different
Improvement of knee motion is a goal of total knee replacement, but restoration of full motion is uncommon. The motion of your knee replacement after surgery can be predicted by the range of motion you have in your knee before surgery. Most patients can expect to be able to almost fully straighten the replaced knee and to bend the knee sufficiently to climb stairs and get in and out of a car. Kneeling is sometimes uncomfortable, but it is not harmful.
Most people feel some numbness in the skin around your incision. You also may feel some stiffness, particularly with excessive bending activities.
Most people also feel or hear some clicking of the metal and plastic with knee bending or walking. This is a normal. These differences often diminish with time and most patients find them to be tolerable when compared with the pain and limited function they experienced prior to surgery.
Your new knee may activate metal detectors required for security in airports and some buildings. Tell the security agent about your knee replacement if the alarm is activated.
Protecting Your Knee Replacement
After surgery, make sure you also do the following:
Participate in regular light exercise programs to maintain proper strength and mobility of your new knee.
Take special precautions to avoid falls and injuries. If you break a bone in your leg, you may require more surgery.
Make sure your dentist knows that you have a knee replacement. Talk with your orthopedic surgeon about whether you need to take antibiotics prior to dental procedures.
See your orthopedic surgeon periodically for a routine follow-up examination and x-rays. Your surgeon will talk with you about the frequency and timing of these visits.
Extending the Life of Your Knee Implant
Currently, more than 90% of modern total knee replacements are still functioning well 15 years after the surgery. Following your orthopedic surgeon's instructions after surgery and taking care to protect your knee replacement and your general health are important ways you can contribute to the final success of your surgery.
For more information about your recovery following knee replacement surgery, take a look at our post-operative protocols.